
Post Procedure Complications
Case Presentation:
You are part of the overnight team that is taking care of a 61 year old male with PMH of HFrEF <20%, DM, ESRD on HD, HTN, HLD who presented for planned CRT-D device implantation. Per signout, the procedure was uncomplicated and the patient is doing well. Overnight, an RRT is called on the patient for BP of 80/50, HR 120s, and O2 saturation on 6L at 94%.
Ask Yourself:
1. Given this patient just had a device implanted, what complications are highest on your differential?
2. What are you looking for on physical exam that might alert you to the diagnosis?
3. What tests do you want to order?
4.What interventions need to happen in order to help stabilize the patient?

Background:
There are three major categories of cardiac implantable electronic devices (CIED), which include the pacemaker (PPM), cardiac resynchronization therapy (CRT), and implantable cardioverter-defibrillator (ICD). As these devices are widely used in cardiology, it is important to understand the indications, differences, and complications associated with each device type.
The Pacemaker
The Pacemaker helps to stimulate electrical impulses within the heart in order to help maintain or restore a functional heart beat, usually in the setting of sinus node dysfunction and high grade atrioventricular (AV) block.
The following are common Class 1 Indications for Pacemakers:
Sinus node dysfunction:
Symptomatic sinus bradycardia or sinus pause
Symptomatic chronotropic incompetence (i.e. inability to achieve 85% age predicted maximal HR with activity)
AV / Bifascicular Block:
Complete 3rd degree AV block with or without symptoms
Symptomatic 2nd degree AV block (Mobitz 1 and 2)
Exercise induced second or third degree AV block
Permanent Mobitz 2 or intermittent 3 degree AV block
Alternating bundle branch block

The pictures above show a patient with a dual chamber pacemaker with the picture on the right highlighting exactly where the pacer wires travel. This patient has a wire in the right atria (pink) and in the right ventricle (green). Note how thin these wires are.
ICD:
The ICD is used to help prevent sudden cardiac death in patients who have had prior sustained VT / VF without reversible causes or who have high risk of developing VT / VF. Notably, ICDs are placed between the muscle and fascia layer under the serratus anterior muscle.
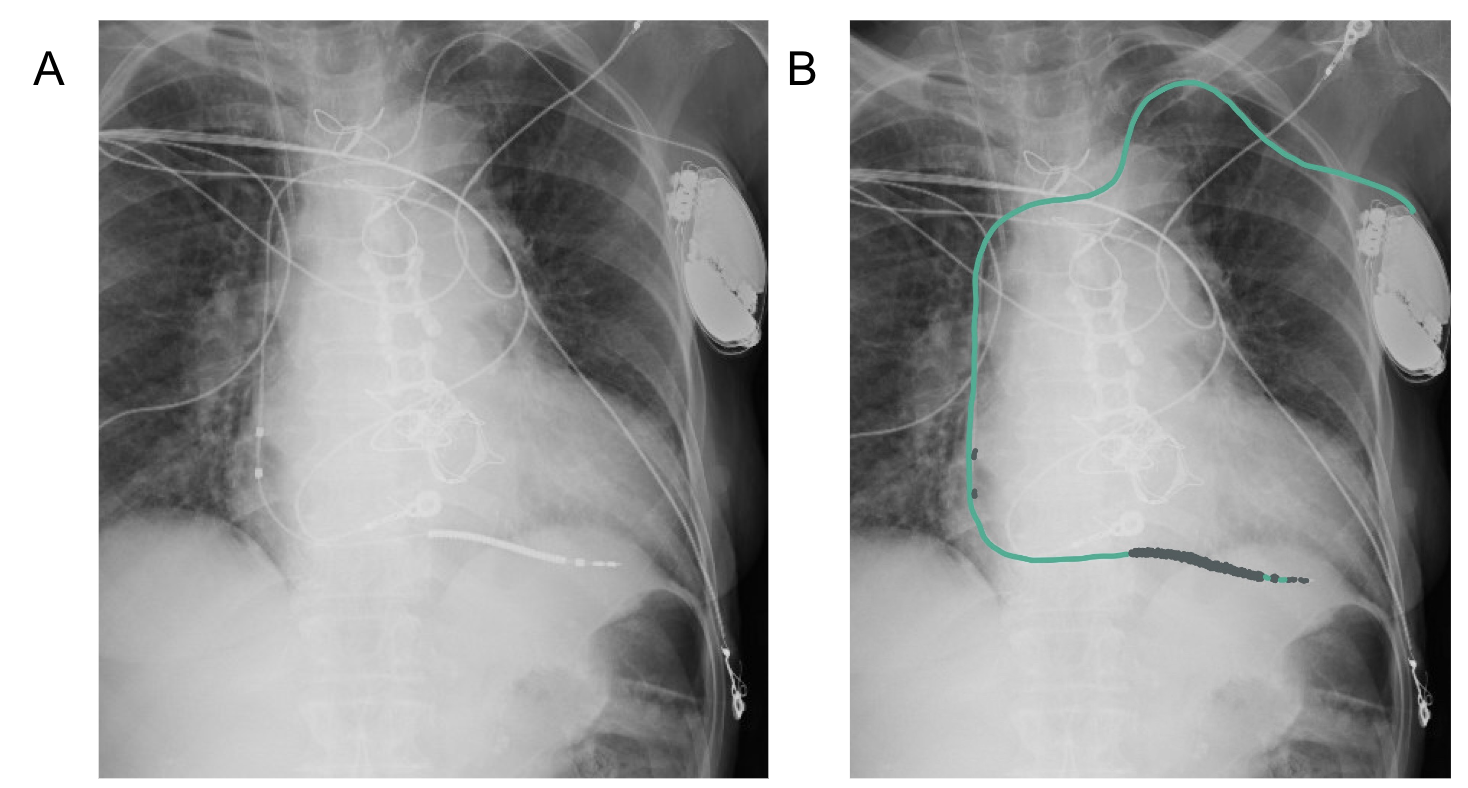
Figure 4A shows a patient with a single chamber defibrillator lead in the right ventricle, highlighted in green in 3B. Notice how this wire is thick (outlined in grey) unlike the thin pacemaker leads (seen in Figure 2) as the defibrillator requires this thicker coil to deliver a shock if needed.
Indications for ICDS are split up into primary and secondary prevention:
Primary Prevention:
Patients who have had life threatening VT/VF despite being treated with optimal medical management
40 days post MI with new EF < 30%
Secondary Prevention:
Patients with a prior episode of resuscitated VT / VF or hemodynamically unstable VT without a reversible cause
EF < 35% despite at least 3 months of GDMT in patient with non-ischemic cardiomyopathy and NYHA Class II +
Sustained VT in patients with known heart disease, whether valvular, ischemic, hypertrophic
Unexplained, abrupt syncope in a patient with EF </= 35% that is presumed to be arrhythmic, in both ischemic and non-ischemic cardiomyopathy
ICDs can also be placed in patients who are at high risk due to
Congenital long QT syndrome with recurrent symptoms
Hypertrophic cardiomyopathy or arrhythmogenic right ventricular dysplasia
Brugada syndrome
Catecholaminergic polymorphic VT
Family history of sudden cardiac death
ICD NOT indicated in patients who have:
VT/VF within the first 48 hours post acute MI.
Reversible causes of VT / VF (i.e. drugs, electrolyte imbalance, ischemia)
Life expectancies < 1 year
Syncope without inducible tachyarrhythmias or structural heart disease
Ability to undergo catheter ablation to prevent further arrhythmias
Cardiac Resynchronization Therapy:
The Cardiac Resynchronization Therapy (CRT device) is used in patients with HFrEF and dyssynchronous ventricular function (seen by widened QRS >120 ms). The CRT will thus simultaneously activate both the LV and RV allowing for more synchronous biventricular function which can ultimately help improve the patient’s heart function, hemodynamic status, cardiac output, and contractility. In order to accomplish this, there is a lead placed in the coronary sinus in order to activate the LV, RV, and right atrium.
Studies have shown that both QRS prolongation and LBBB were associated with increased mortality in patients with HFrEF. Notably, RBBB alone has not been linked to increased mortality since it does not cause the same hemodynamic dyssynchrony as LBBB.

The cartoon picture above shows a CRT with the RA lead (pink), RV (green), and LV lead (blue). Use this picture to compare to the CXR on the left to help you visualize where the leads are and how they are placed in the chest.
Considerations for CRT include EF, NYHA class, presence of LBBB, QRS duration, and need for LV pacing. Patients should be considered for CRT when:
EF < 35% despite at least 3 months of GDMT or despite attempt at treating reversible causes (i.e.ischemia, tachycardia induced cardiomyopathy, etc) or are 40 days post MI if
QRS > 130 with LBBB and NYHA II + symptoms
QRS > 150 with LBBB, NYHA I +, and ischemic cardiomyopathy
QRS > 150 with no LBBB and NYHA 3 +
Patients with EF 35-50% and need for >40% ventricular pacing
Patients with EF 35-50% and QRS > 150 ms with LBBB and NYHA Class III+ despite treatment with GDMT for at least 3 months or treatment for reversible causes of heart failure

The picture on the left shows a CXR of a patient with a CRT-D. The picture on the right shows the RA lead (pink), RV lead (green), and the blue lead (i.e. the lead that goes through the coronary sinus to stimulate the LV). Note the thick defibrillator wire, making this CRT and CRT-D. (rather than a CRT-P, pacemaker).
Considerations for CRT include EF, NYHA class, presence of LBBB, QRS duration, and need for LV pacing. Patients should be considered for CRT when:
EF < 35% despite at least 3 months of GDMT or despite attempt at treating reversible causes (i.e.ischemia, tachycardia induced cardiomyopathy, etc) or are 40 days post MI if
QRS > 130 with LBBB and NYHA II + symptoms
QRS > 150 with LBBB, NYHA I +, and ischemic cardiomyopathy
QRS > 150 with no LBBB and NYHA 3 +
Patients with EF 35-50% and need for >40% ventricular pacing
Patients with EF 35-50% and QRS > 150 ms with LBBB and NYHA Class III+ despite treatment with GDMT for at least 3 months or treatment for reversible causes of heart failure
The CRT comes in two flavors, namely the CRT-P (pacemaker) and CRT-D (defibrillator). Generally, patients > 75 years old without CAD and are pacemaker dependent tend to do better with CRT-P. Since CRT-D devices are bigger, more expensive, and have increased risk of infection, CRT-P is preferred unless the patient also has an indication for an ICD.

This EKG shows the precordial leads in a patient with a left bundle branch block. Notice how the QRS is wider than the normal 120 msec (i.e. 3 small boxes).
Device Complications:
While it has been shown that device related complications are <10% within the first few years after implantation, it is important to understand and recognize the risks as the majority of complications occur immediately after the procedure and within the first year post implantation.
Infection:
The main culprits are usually gram positive skin microbiota. If infection is suspected, blood cultures, TEE, CT, and PET scan can be done. In order to prevent infection, patients are given prophylactic first generation cephalosporins like Cefazoline 2g prior to the procedure. For additional prevention, the device is put in an antibiotic infused pouch (courtesy of Medtronic).
Cardiac Perforation:
This is a very rare (<0.4% of all device implantations) and deadly complication that can occur secondary to cardiac puncture by wire or leads during the procedure and can ultimately cause pericardial effusion or tamponade (picture from Osmosis).
Pocket Hematoma Formation:
The most important thing to remember here is to APPLY PRESSURE and do NOT try to drain the pocket as introducing foreign objects into the skin increases the risk of infection.
Pneumothorax:
Depending on size and hemodynamic status, may require needle decompression and chest tube (JetEM).

Antibiotic infused pouch, courtesy of Medtronic

Subxiphoid view of pericardial effusion (noted by the astrix) causing cardiac tamponade.

Picture of pocket hematoma courtesy of ClinMed

Picture of pneumothorax, courtesy of JetEM
Dislodgement and malfunction of the device:
Devices and leads can migrate on their own or because the patient inadvertently causes the device to move by twiddling with the device (AKA “Twiddler’s Syndrome). Misplaced devices and leads can prevent the device from working properly and may ultimately lead to misfiring or poor device capture.
Pacemaker Mediated Cardiomyopathy:
Patients who have frequent RV pacing can develop systolic dysfunction as the frequent pacing can cause ventricular dyssynchrony. If this occurs, the patient either needs device reprogramming to reduce RV pacing or upgrade to CRT (with a CS lead or conduction system pacing).
Nerve disruption:
The two main nerves that can be damaged or disrupted are the phrenic nerve during CRT placement and the long thoracic nerve when the ICD is placed under the serratus anterior muscle. As such, side effects include diaphragmatic discoordination or winging of the scapula, respectively.
Inappropriate shocks:
Unfortunately occurs when ICDs are oversensing, worse in patients with atrial fibrillation and hypertrophic cardiomyopathy. The ICD must be turned off, which can be done with the extracardiac magnet.
Damage to the endocardial architecture:
An example of this is tricuspid regurgitation due to lead impedance or damage from procedure. Formal TTE can be ordered to determine any damage that may have been done to either the valves or the endocardium itself.
Pacemaker Syndrome:
This phenomenon is seen most commonly with single chamber devices in which there is only sensing and pacing in one chamber. As a result, there is a disconnect between the atria and ventricles, causing poor cardiac coordination and resulting in reduction of cardiac output. EKG will show dyssynchrony between the P waves and QRS. Patients will most likely need to be upgraded to a dual chamber device to avoid any further complications.

This figure shows the pathways of the Long Thoracic (maroon) and the Phrenic nerves (orange). From this picture, we can see how these nerves can be damaged during device implantation

The figure below (courtesy of Clinical Cardiology) shows how device leads can damage cardiac structure and cause tricuspid regurgitation.

The figure below (courtesy of The British Journal of Cardiology) depicting Pacemaker Syndrome with lack of atrial capture
Back to the Case:
1. Given this patient just had a device implanted, what complications are highest on your differential?
Knowing which type of device the patient received is important to understanding potential complications. As a CRT-D involves 3 wires, one of which goes through the coronary sinus, it has the highest risk of complications. As this patient is quickly decompensating shortly after his procedure, the most important things to rule out are cardiac tamponade secondary to cardiac perforation, pocket hematoma, and pneumothorax.
2. What are you looking for on physical exam that might alert you to the diagnosis?
Make sure listen to heart and lung sounds and check JVD, which might alert you to potential tamponade or pneumothorax. Also make sure to assess the patient’s generator pocket to ensure there is not a massive hematoma that is forming. Most importantly, make sure to feel the temperature of the patient’s extremities in case this patient is developing shock that may require pressors.
3. What tests do you want to order?
Definitely get a STAT CXR, EKG, and CBC. Although it is very unlikely to be septic so quickly due to device infection, you can also consider getting blood cultures and a lactate as well. If possible, try to perform a bedside POCUS, specifically with a subxiphoid view that may allow for better visualization of any pericardial effusions.
4. What interventions need to happen in order to help stabilize the patient?
If this is cardiac tamponade, the patient needs both fluids (as he is preload dependent) and pericardiocentesis. If this is a pocket hematoma, you need to apply pressure to the hematoma to prevent it from increasing in size and transfuse for a hgb > 7. However, if the patient has a new pneumothorax, he will require emergent chest tube placement.
Further Learning:
Resident Responsibilities:
Ensure prophylactic antibiotics are ordered prior to device implantation
Make sure patients get AP and lateral CXR post procedure to ensure proper generator and lead placement. Also make sure to look for any signs of pneumothorax.
Try to enforce minimal arm movement post procedure and that the patient wears the sling provided to prevent device migration or pocket hematoma from forming.
If a pocket hematoma does develop, please ensure that it is properly wrapped with enough pressure to prevent further growth. Whatever happens, DO NOT ASPIRATE HEMATOMA.
Attending and Fellow Pearls:
Patients actually have a higher chance of bleeding when being bridged than when they are just continued on their home warfarin. It is better to keep a patient on their home warfarin or DOAC than start them on a heparin drip as heparin drips had higher rates of hematoma pocket formation!!
Any time a pocket becomes infected and the device needs to be replaced, the new device will be implanted in a different spot (i.e. on the right side instead of the left)
If patients with devices are having any surgeries that occur above the iliac crests, they will need cardiology consulted to change device settings
When patients get surgery, devices need to go into asynchronous mode which allows the device to pace and NOT sense. This ensure that the cautery use during the surgery does not affect the heart’s pacing.
Putting a magnet on an ICD only stops the defibrillator! It does NOT stop the device from pacing!
High Yield Trials for Further Reading:
CARE-HF trial–The first study to show significant reduction in mortality for CRT therapy for patients with QRS > 150 ms with increased LV function.
MOST, PACE, CTTOP trial- Pacemaker syndrome
Danish Trial- New report questioning the need for prophylactic ICDs in patients with non-ischemic cardiomyopathy
REPLACE Registry– a prospective multicenter study of patients undergoing device reimplantation. Investigators from this study made the REPLACE DARE Mortality Risk Score.
BRUISE Control Trial–the largest randomized trial of antithrombotic treatment strategies in patients undergoing device implantation Found that patients were more likely to have bleeding associated complications when bridged from warfarin to heparin rather than just remaining on warfarin.
BRUISE Control 2 found that there was no significant difference of bleeding for patients who were continued on a NOAC vs those who had NOAC stopped.
How’d we do?
The following individuals contributed to this topic: Rebecca Garber, MD, Isaac Whitman, MD
Chapter Resources
Meta analysis of complications related to device implantation
Goes over the specifics of how the device is implanted in each situation
Pacemaker indications
CRT-P/D
Pacemaker syndrome
https://www.sciencedirect.com/science/article/abs/pii/S0002870302000261?via%3Dihub
The longer the QRS, the higher the mortality
LBBB > RBBB
Factors causing de novo infection
Up to 50% of patients who receive CEID are on anticoauglation
Coronary sinus dissections
https://www.washingtonhra.com/pacemakers-icds/cardiac-resynchronization-therapy-crt.php
Picture
https://radiologyassistant.nl/cardiovascular/devices/cardiovascular-devices
CXR device pictures