
Pump Problems
Case Presentation:
74yo woman with a history of HFrEF (25-30%) and CKD 3 is admitted to the CCU service for acute decompensated heart failure. Patient was initially diuresing well but developed AKI, hypotension to 80s/50s, and lactic acid of 4.2. Later on rounds, it is decided that the patient will undergo right heart catheterization with pulmonary artery (PA) catheter (Swan-Ganz) placement for closer hemodynamic monitoring.
Ask Yourself:
Questions:
1. What arse the indications for placement of a PA catheter in this patient?
2. How do I get the data and how do I interpret it?
3. What complications should I look out for in patients with a PA catheter in place?

What is cardiogenic shock?
Think signs of end-organ hypoperfusion and congestion. Blood pressure may not be low!
Patients can present anywhere on this spectrum of cardiogenic shock
Beware of Normotensive Cardiogenic Shock!!Although the blood pressure may look normal, the body is still not getting perfused well. This can be seen clinically by an elevated lactate, poor urine output (due to poor renal perfusion), and cold extremities.


Figure 2: Depicting different stages of cardiogenic shock. Courtesy of Society for Cardiovascular Angiography and Interventions
Figure 3: Shows the Forrester Classification of different classes of acute decompensated heart failure. The different classes, including warm and dry (the best category as it depicts volume overload but good perfusion) to cold and wet (worst because it means volume overload with poor perfusion) and how to treat them (with diuretics vs inotropic agents).
How to Differentiate Cardiogenic vs Septic Shock:
When patients are in shock, they have increased metabolic states. As such, they require more energy, aka ATP. Since aerobic metabolism gives the body more ATP, the body will try to deliver more oxygen. Figure 4 depicts the difference between cardiogenic vs septic shock and how the body tries to compensate in each case. The body has a few ways to help accomplish this:
1. Increasing cardiac output (CO) by increasing heart rate (HR) and stroke volume (SV).
Cardiogenic shock: the heart cannot generate enough force to increase stroke volume, so it must rely on the heart rate to increase CO. Clinically this is seen by narrow pulse pressures and is why patients in decompensated heart failure do very poorly with newly added beta blockers.
Septic shock: both HR and SV increase. Plus, the decreased systemic vascular resistance (SVR) allows for an increased CO.
2. Increasing oxygen absorption from the passing red blood cells
Cardiogenic shock: the body will try to take every last O2 from the red blood cells (RBCs).
Septic shock: given the increased CO, the tissues don’t have enough time to take O2 from the passing RBCs since they’re moving so quickly
3. Anaerobic metabolism
When all else fails, the body will go into anaerobic metabolism. This can be seen clinically with a rising lactic acid (LA) as this is the byproduct of anaerobic metabolism.

When to use and not use a PA catheter:
Indications
To guide management in cardiogenic shock
To help us accurately determine how well mechanical support devices, such as Impellas or Balloon Pumps, are augmenting cardiac output and perfusion
Differentiation between the type of shock in patients with potentially mixed picture
Defining volume status in unclear clinical pictures and severe shock
Assessment of pulmonary hypertension
Contraindications
Infection at catheter insertion site
RV assist device
Relative contraindications
Coagulopathy
LBBB due to concern for complete heart block since the catheter can irritate the right side of the heart and cause a RBBB
Severe Tricuspid or pulmonic stenosis (VERY rare)
The Pulmonary Artery Catheter aka The Swan:
A PA catheter (AKA Swan-Ganz) can be used to directly measure pressures inside the heart. This catheter is a long, balloon-tipped catheter that gets inserted usually in the internal jugular vein and threads down the SVC into the RA, through the RV, and into the pulmonary artery, where the balloon can be inflated and measure pulmonary capillary wedge pressure, a conduit for left atrial pressure (Figure 5). We expect a different pressure tracing depending on location of the catheter

Thermistor: Intended for thermodilution measurements (CO and CI) as it has a temperature sensitive wire that can help measure temperature change.
Proximal Injection Port: The most proximal port that can be used for infusing medications. Also intended for the cold thermodilution fluid and for measuring central venous pressure (CVP)
Right Atrium (RA) Port: Power plug for the heating filament and used for infusion.
Pulmonary Artery (PA) / Distal Port: Meant for measuring PA pressure and mixed O2 saturation sampling (via VBG)
Balloon Port: Has the balloon attached to the end. This balloon can be inflated up to 1.5mL

This picture (Figure 6) depicts waveforms seen as the PA catheter is advanced through the heart (Figure 5). These waveforms are taken from the right atrium (RA) at point A to measure CVP, right ventricle (RV) at point B, pulmonary artery (PA) at point C, and then right after the balloon is inflated (AKA wedged) to correlate to the LA pressures at point D.
Refresher:
Refreshers:
Obtaining accurate pressure readings depends on zeroing the transducers at the level of the RA (mid thorax) when the patient is laying flat (figure 7) and ensuring there is no air in the lines.
Remember normal pressures in the heart with a nice mnemonic “nickel-quarter-nickel-quarter-dime.” This correlates to RA-RV systolic-RV diastolic-PA systolic-PA diastolic/Wedge.
Wedge pressure correlates with LA pressure which correlates with LV end diastolic pressure (LVEDP). This helps us differentiate pre- and post-capillary pulmonary hypertension (i.e. is the high pressure from the lungs or the heart)
High wedge pressures tell us the patient is overloaded


Figure 7: Remember that in order to obtain accurate pressures, the patient needs to be laying flat!
Figure 8: Shows where to look for the CVP on the patient’s monitor. Remember, normal CVP is ~8!
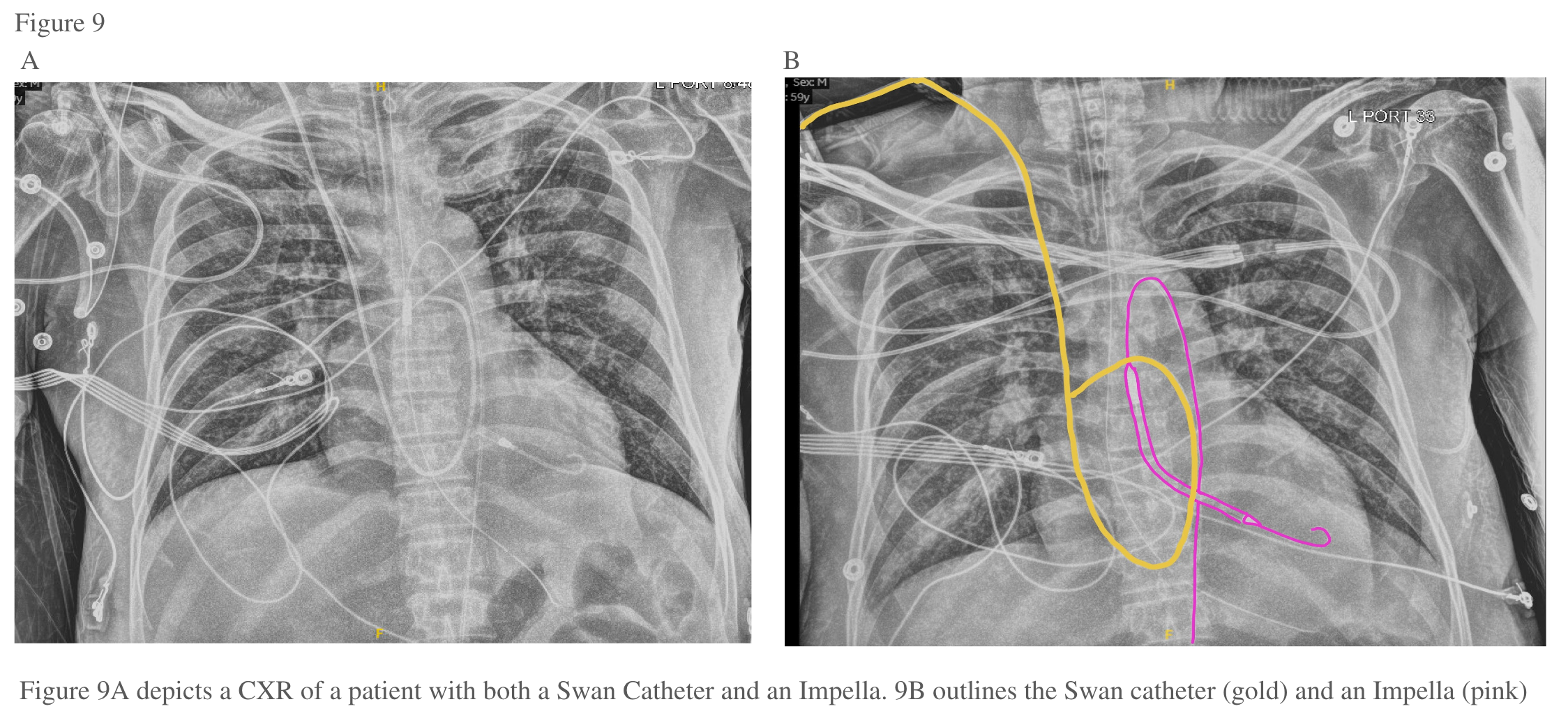
Positioning of the Catheter–Should be assessed with CXR daily:
Fick vs Thermodilution:
We can use the PA catheter (AKA Swan-Ganz) to help us measure cardiac output (CO) and cardiac index (CI). This can be achieved by either using Thermodilution or the Fick equation:
Fick: There are two main ways to estimate Fick:
Mixed venous O2 saturation — uses oxygen concentration in pre- and post- oxygenated hemoglobin (hgb). In order to use this equation, we must know the patient’s height, weight, hemoglobin, the O2 saturation on the hgb right at the PA before it gets reoxygenated (i.e. mixed venous O2 saturation–MvO2–which we get from the VBG), and the O2 saturation after the hgb is oxygenated (SaO2 on the ABG). Figure 10 shows how those calculations are generated.
Continue Cardiac Output Estimation – uses information from the arterial pressure wave to estimate cardiac output and cardiac index by assessing the stroke volume (SV) (i.e. area under the curve) and heart rate ( SVxHR = CO). As evidenced by the name, this is a continuous measurement as is usually assessed via the monitors at bedside (Figure 11).
Thermodilution:
This is done only in the cath lab. We measure the temperature changes of fluid as it passes along the catheter within the heart. The fluid is released within the RA and then measured by the thermistor in the pulmonary artery (PA). The better the CO, the faster the blood will flow and the less the temperature will change. In contrast, the worse the CO, the more time the fluid has to warm up and the more the temperature will change from point A to point B.


Putting it all together–
Courtesy of Cardio Nerds

Swan Sheet— To be filled out EVERY time a patient has a Swan

Back To The Case:
1. Why place a PA catheter in this patient?
The placement of a PA catheter in this patient is dictated primarily by the patient’s clinical picture concerning for cardiogenic shock. Placing a PA catheter to directly assess filling pressures, guide the use of inotropes/inodilators/pressors/mechanical support, and assist in diuresis strategy to improve the patient’s clinical condition. PA catheters, while not recommended for the routine use of heart failure management, can be used in patients with cardiogenic shock and have shown to improve mortality in these patients.
2. How do I get the data and interpret it?
Make sure the catheter is zeroed at the level of the RA (should be checked every time measurements are taken). Once you have the data for RA pressure, PA pressures, and wedge pressure you can make some calculations to tell you the patient’s volume status, cardiac output, afterload (SVR), and pulmonary vascular resistance (PVR). Patients with low cardiac output (by Fick and/or thermodilution) may benefit from inotropes. High afterload may benefit from additional afterload reducing meds (e.g. ACE/ARB/ARNI/hydralazine/nitroprusside). Patients with high PVR may benefit from specific therapies for pulmonary hypertension and can give you a sense of biventricular failure with the calculation of the PAPI
3. What should I be on the lookout for in caring for patients with these in place?
Positioning of the catheter is of utmost importance. If the catheter is in the wrong place, it won’t give you accurate numbers and you won’t be able to make accurate calculations. Be cautious to not leave the PCWP balloon inflated for too long as you run the risk of erosion/PA injury/pulmonary infarct. Always be sure to note the positioning of the catheter to ensure it has not moved significantly.
Further Learning:
Resident Responsibilities
Placing a PA catheter will be helpful in managing patients with cardiogenic shock, assessing volume status, and treatment of severe pulmonary HTN
Please make sure to have CO and CI (both mostly done using Fick via the MvO2) for rounds on ALL patients who have PA catheters. See next sheet.
Ensure proper placement of the catheter at least daily with a CXR. Note how far the catheter is in.
ONLY FELLOWS ADVANCE / RETRACT THE CATHETER AND INFLATE BALLOON!!
The balloon should ALWAYS be deflated after measurements are taken. Don’t leave it inflated!!
Attending and Fellow Pearls
Valve pathologies can make pressure readings more difficult to interpret
Patients with PA catheters are quite sick and need very close monitoring.
The threshold to call for help is very low if you are having issues with obtaining data from the catheters or the numbers are not making sense
Decisions made based on the information obtained from the PA catheter should be made with the fellow/attending
Further Reading
ESCAPE Trial: RCT from 2005 demonstrating no significant difference in days alive out of hospital or mortality at 6 months. One of the main reasons why we don’t routinely use PA catheters in ADHF
The ESCAPE Investigators and ESCAPE Study Coordinators. Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness - The ESCAPE Trial. JAMA. 2005;294(13):1625-1633. doi:10.1001/jama.294.13.1625
“Hemodynamics for the Heart Failure Clinician”: Excellent overview of interpretation of PA catheter tracings
Hsu S, Fang JC, Borlaug BA. Hemodynamics for the Heart Failure Clinician: A State-of-the-Art Review. J Card Fail. 2022;28(1):133-148. doi:10.1016/j.cardfail.2021.07.012
Two retrospective trials suggesting benefit of PA catheter placement in patients with cardiogenic shock:
Garan AR, Kanwar M, Thayer KL, et al. Complete Hemodynamic Profiling With Pulmonary Artery Catheters in Cardiogenic Shock Is Associated With Lower In-Hospital Mortality. JACC Heart Fail. 2020;8(11):903-913. doi:10.1016/j.jchf.2020.08.012
Right Heart Catheterization in Cardiogenic Shock Is Associated With Improved Outcomes: Insights From the Nationwide Readmissions Database. doi:10.1161/JAHA.120.019843
How’d we do?
The following individuals contributed to this topic: Ryan Khalil, MD, Mayank Kansal, MD
Chapter Resources
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001063
2022 AHA/ACC/HFSA heart failure guidelines
Overview of cardiogenic shock
SCAI classification of cardiogenic shock
State of the art review of hemodynamics
Brief overview of PA catheter placement
https://www.ahajournals.org/doi/10.1161/CIRCHEARTFAILURE.120.007099#F1
Use of PA catheter data for appropriate classification of cardiogenic shock
Cardionerds Podcast on RHC evaluation in cardiogenic shock