
Inflammatory Diseases
Case Presentation:
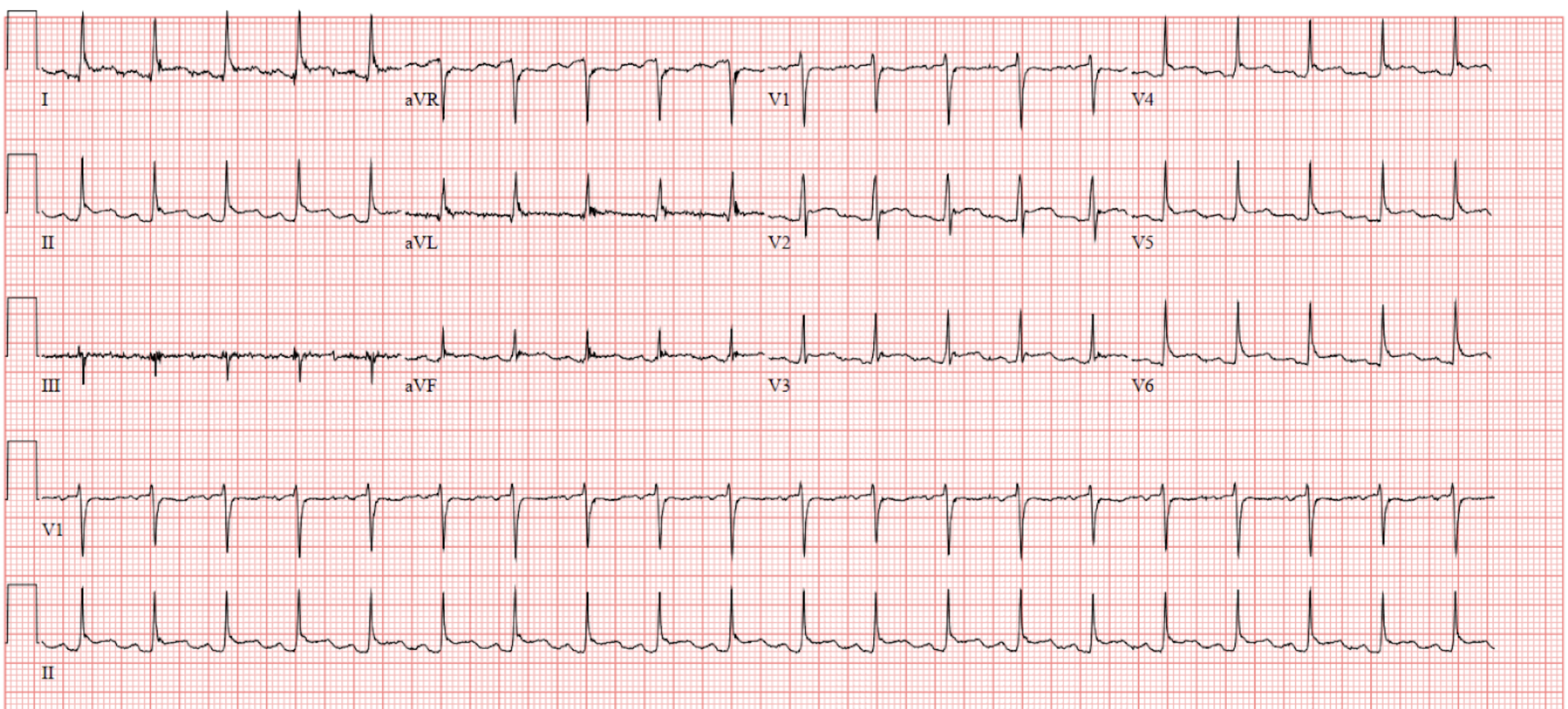
A 30 year old female with a history of SLE and asthma presents to the ED with acute onset of sharp, substernal chest pain in the setting of a mild, nonproductive cough for the past ten days. The chest pain is described as sharp, without radiation to the arms or neck, improves when the patient sits up, and worsens with deep breaths. In the emergency department, the patient’s vital signs are significant for a heart rate of 120 and temperature of 102.8, with labs notable for a 2 hour high-sensitivity troponin trend of 265 -> 160 and a WBC count of 15,400 (85% neutrophils). A scratchy, velcro-like sound is appreciated at the left sternal border. ECG is obtained on presentation to the emergency department and shown below.
Ask Yourself:
What is notable about this EKG?
What do you think the patient is presenting with? What are the etiologies of this disease?
What is the management of this disease? Would you think of giving her steroids?
What are the main complications of this disease?
In this lesson, we will be focusing Pericarditis:
Acute Pericarditis Diagnosis
The diagnostic criteria for acute pericarditis are based on a combination of clinical findings, electrocardiographic (ECG) changes, and imaging studies. The most commonly used diagnostic criteria are those developed by the European Society of Cardiology in 2004:
Clinical symptoms: Chest pain is the hallmark symptom of acute pericarditis. Chest pain characteristic of pericarditis is typically sharp and pleuritic in nature, and worsens with deep inspiration, coughing, and lying down.
Chest pain may resemble that of myocardial ischemia (radiation to shoulders, steady quality)6
In more subacute forms of pericarditis (uremic, TB) pain may be minimal
ECG changes: The ECG is a key tool in diagnosing acute pericarditis. The characteristic ECG findings are discussed below, but classically include diffuse ST-segment elevation often accompanied by PR-segment depression.
Pericardial effusion on TTE: present in 2/3 of cases3, typically small, hemodynamically insignificant
Pericardial friction rub: A pericardial friction rub is a scratchy, grating sound that occurs when the inflamed pericardial layers rub against each other during the cardiac cycle.
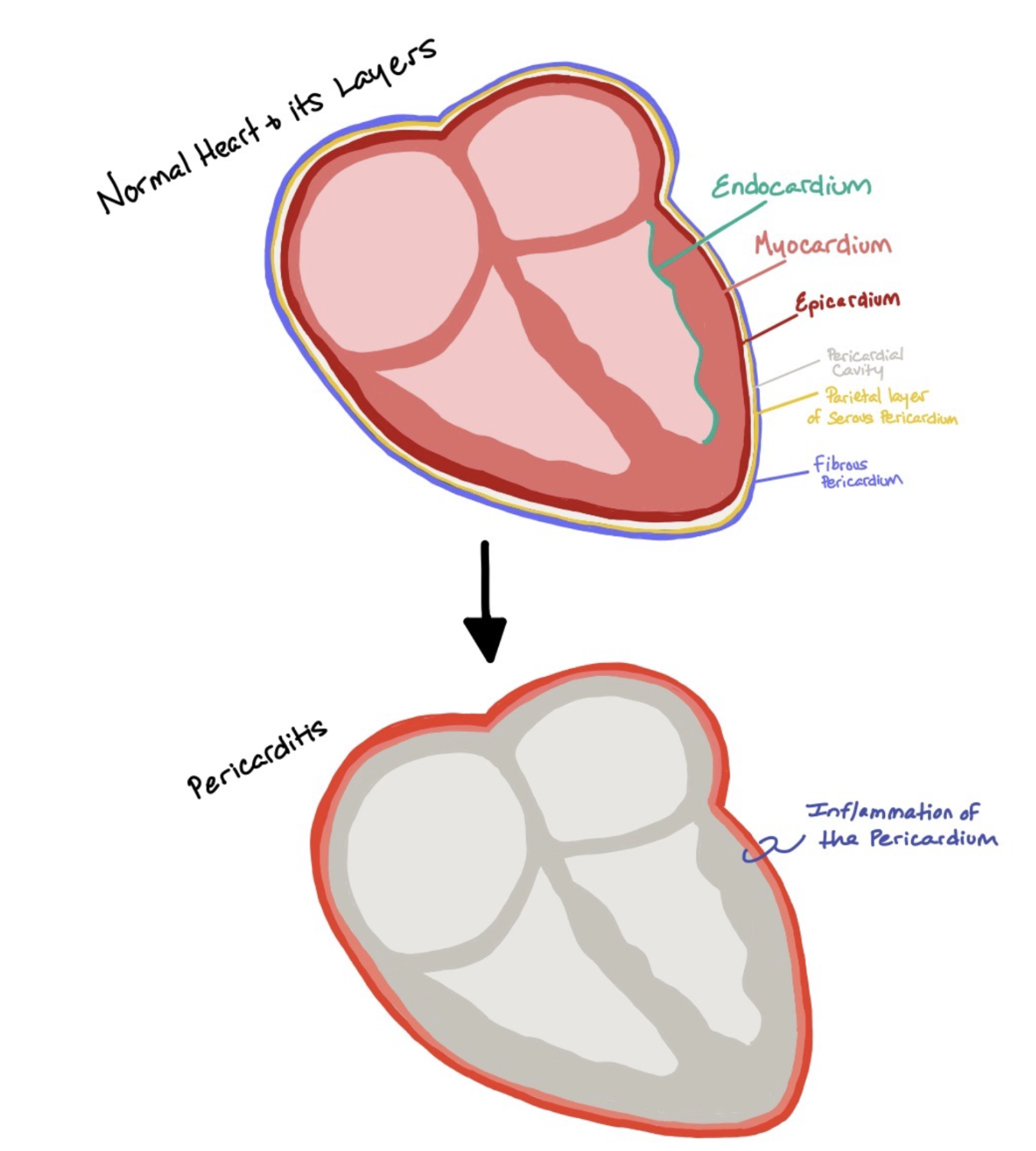
This picture demonstrates the normal layers surrounding the heart from the fibrous pericardium to the endocardium. During pericarditis, patients have inflammation of the pericardial layer, as represented by the red outline surrounding the heart.
Given the diagnostic criteria, basic evaluation for suspected pericarditis should include a TTE, ECG, and possibly troponin level. For a definitive diagnosis of acute pericarditis to be made, a patient must have at least two of the above criteria. In addition, it is critical to rule out other causes of chest pain and ST-segment elevation on ECG, such as acute myocardial infarction and pulmonary embolism.
If the suspected diagnosis of pericarditis cannot be confirmed based on the above criteria, strategies to help differentiate pericarditis from other diagnoses include frequent repeat ECGs and auscultation (ECG changes and friction rub may be transient) and measurement of troponin levels (can help distinguish pericarditis from myopericarditis or myocarditis). In some cases, cardiac MRI can also be helpful, as late gadolinium enhancement of the pericardium can suggest pericarditis. In some instances, you may need to have the patient get a coronary angiogram to distinguish pericarditis from a STEMI.
EKG Findings in Pericarditis:
Findings suggestive of pericarditis (rather than ST elevation myocardial infarction)
Spodick’s Sign: Below, see the down-sloping of the TP segment (arrows), seen in ~20-30% of pericarditis cases

PR depressions (seen below), is present in ~60% of pericarditis cases

Pericarditis vs. STEMI:
Differential Diagnosis
The differential diagnosis includes any conditions which can cause chest pain characteristic of pericarditis, including PNA, pleurisy, PE, GERD, and costochondritis. The most critical step is to differentiate pericarditis from other causes of elevated ST segments:
Myocarditis: On ECG, myocarditis may have diffuse ST elevations. Myocarditis will most likely have more elevated troponin levels than pericarditis (although there can be involvement of the myocardium in myopericarditis). Most importantly, myocarditis will have global or regional/segmental systolic dysfunction, while this is not an expected finding in pericarditis.
ST segment myocardial infarction (STEMI): Unlike pericarditis, STEMIs will usually have ST elevation in a particular coronary distribution with reciprocal depressions.
Findings suggestive of ST elevation myocardial infarction (rather than pericarditis)
Reciprocal ST depression (aside from those in aVR or V1, which are normal)
Reciprocal depressions are seen in 66% of STEMI cases, as opposed to only 2% of pericarditis cases2
In the case EGC, note absence of ST depression in leads other than aVR or V1
Greater degree of ST elevation in III compared to II
In case ECG, note prominence of ST elevation in II vs absence in III
Convex upwards quality of ST elevation (e.g. tombstones, as opposed to concave)
Below ECG has convex (classic tombstone appearance) ST elevations (precordial leads), while the case ECG has concave ST elevations (best seen in lead II). This is less consistent with pericarditis.

It is critical to exclude other causes of ST elevations, particularly ST elevation myocardial infarction, before concluding on the diagnosis of pericarditis. Despite classical ECG findings taught in medical school, the distinction can be challenging. This is more likely to be a distinction which will be made in the ED, but is important for internal medicine residents to be familiar with these findings as well. The initial diagnostic imperative when reviewing an ECG with ST elevations is to rule out ST elevation myocardial infarction.
Etiologies of Pericarditis:

This figure shows a normal heart with all its layers (top) and a heart with pericarditis (middle). The bottom picture depicts pericarditis causing a pericardial effusion due to all the inflammation occurring from the inflammation of the pericardial sac. If too much fluid accumulates within the pericardial sac, this can cause tamponade due to the increased pressures from the fluid accumulation.
In the majority of cases in developed countries, 80-90% of cases are idiopathic, and assumed to be secondary to a viral process. In developing countries, mycobacterium tuberculosis is the most frequent cause of acute pericarditis. Despite the infrequency of specific alternate etiologies of pericarditis, it is imperative that these cases are recognized, as management of specific etiologies of pericarditis may be markedly different than treatment of typical idiopathic cases. Common specific etiologies include post-cardiac injury syndromes (e.g. after CABG, PCI etc.), connective tissue disease (especially SLE), malignancy, hypothyroidism, and rare autoinflammatory conditions (FMF, TRAPS); specific infectious etiologies include TB, Lyme disease, parvovirus B19, EBV, and purulent pericarditis (s. aureus, strep species).
Findings associated with/suggestive of a specific etiology3,4 -> if you see these, consider a broader workup, which may include autoimmune serologies, blood cultures, and sampling of pericardial fluid, among other testing,
Fever >38°C
WBC >13,000
Large (>20mm width) pericardial effusion
Poor response to typical treatment with NSAIDs + colchicine
Associated anemia
Post-myocardial infarction syndromes (these are now less common given early PCI limiting transmural infarcts)
Early post MI pericarditis: occurs 2-4 days after MI
Dressler Syndrome: immune-mediated phenomenon which occurs weeks-months post-MI
Complications of Pericarditis:
Tamponade
Tamponade is the most acutely concerning complication of pericarditis. Only 3% of pericarditis cases will involve large effusions, and the majority of cases will have small, hemodynamically trivial effusions. Tamponade can be diagnosed by recognizing Beck’s triad and via specific TTE findings.
Recurrent Pericarditis
The prognosis of idiopathic acute pericarditis is generally excellent, however up to 30% of patients may experience recurrence of symptoms. Recurrence is thought to be an immune mediated phenomenon and presents similarly to acute pericarditis. In cases with frequent recurrence , autoinflammatory conditions such as Familial Mediterranean Fever and TNF Receptor Associated Periodic Syndrome should be considered. A brief discussion of the management of recurrent pericarditis is below.

In this figure, we can see how pressure tracings change based on cardiac pathologies. All pressure tracings should be looked at with respect to the EKG to know which part of the cardiac cycle the patient is in. In the normal tracing (purple) we can see the A wave (right atrial contraction), C wave (tricuscpid cusps buldging into the right atrium), X descent (right atrial relaxation), the V wave (rapid filling of the right atrium), and the Y descent (early diastole and ventricular filling). When patients have tamponade (maroon), there is impared flow from the right atrium to the right ventricle due to increased pressures around the right ventricle. As a result, the Y descent will flatten out. In constrictive pericarditis (pink), there is increased atrial pressure with rapid and limited filling, which will cause a notable increase in both the X and Y descent.
Constrictive Pericarditis
This is relatively common (20-30% of cases) when pericarditis is secondary to TB infection, but can be seen on other causes of pericarditis or mediastinal inflammation. Clinical findings are relatively nonspecific (fatigue, decreased exertional tolerance, dyspnea etc.) and the condition can be diagnosed via suggestive TTE findings or on a CT scan.
Pathophysiology: Occurs due to obliteration of pericardial cavity and formation of granulation tissue and scarring within the pericardial cavity, which may eventually calcify.
Physiologic alterations: ventricular filling is reduced in late diastole (when the elastic limit of the pericardium, impeded by calcification, is reached), but normal in early diastole. End diastolic pressure in ventricles, atria, pulmonary and systemic veins will all be similar. On pressure waveforms, a prominent Y descent is seen (reflects rapid early ventricular filling).
Clinical presentation: Kussmaul’s sign is a classic sign (venous pressure does not decline during inspiration). Increased abdominal girth, edema, and nonspecific fatigue/weakness are common; patients often appear chronically ill. Congestive hepatopathy, ascites, and jaundice are also common and can lead to misdiagnosis as hepatic cirrhosis.
ECG – commonly displays low voltage QRS complexes
TTE – will often demonstrate a thickened pericardium with pericardial calcification. Doppler will demonstrate exaggerated respiratory variation in flow velocity (respirophasic changes in mitral and tricuspid inflow). Inspiration: leftward shift of the ventricular septum with reduced flow across the mitral valve. Simplistically, the pulmonary veins basically get “clamped”, so there is less flow into the LA/LV
Expiration: rightward shift of the ventricular septum and relatively increased flow across the mitral valve

Constrictive Pericarditis Right Heart Cath:
Right heart catheterization is the definitive diagnosis! When this is performed, it will show elevated and equal pressures throughout the heart, as well as a cardiac output and pulsus paradoxus. When looking at the pressure tracings, you will see the Square Root Sign caused by a prominent X descent (from elevated right atrial pressures) and prominent Y descent (caused by rapid atrial emptying with increased early diastolic filling).
Treatment:
Typical management of idiopathic pericarditis includes NSAIDs and colchicine. Glucocorticoids may be used as a second or third line option but are not preferred due to well-established increased risk of recurrence. Recurrent pericarditis is often initially managed similarly to acute pericarditis, though the role of therapies such as IL-1 blockers (anakinra) is expanding on the basis of new clinical trial date. The management of specific etiologies for pericarditis is beyond the scope of this guide, however generally would be etiology-guided (e.g. glucocorticoids for SLE).
NSAIDS
Optimal duration and effectiveness have not been clearly established. Typical regimens include aspirin (750-1000mg q8h), ibuprofen (600-800mg q8h), or indomethacin (25-50mg q8h) for 1-2 weeks, or as per clinical response. Consider giving a PPI for ulcer prophylaxis.
Colchicine
Multiple clinical trials (COPE, ICAP) have established the benefit of colchicine in relief of acute symptoms, but particularly in prevention of recurrent pericarditis. Typical regimen includes 0.5-1.2mg colchicine in one of divided doses for 3 months.
Glucocorticoids
Unless there are contraindications to other treatments (or failure of other treatments in recurrent pericarditis), glucocorticoids are not recommended. Studies4 demonstrate increased risk of recurrent pericarditis in a dose dependent fashion. However, ECS6 guidelines suggest addition of steroids (along with continuing NSAIDs, colchicine) in refractory cases; moderate doses (0.2-0.5mg/kg prednisone) for several with a gradual taper (over 2-4 months) preferred compared to higher dose (e.g. >1mg/kg) treatment.
Briefly, the management of recurrent pericarditis should including resuming NSAIDs at dose effective for initial presentation, along with colchicine (which has been established as effective in studies specifically looking at recurrent pericarditis. As above, glucocorticoids should be avoided unless refractory; patients who require glucocorticoids for recurrent pericarditis often may become dependent on them for relief. Newer approaches which have gathered some evidence in RCTs include IL-1 blockers (anakinra). In refractory cases, pericardiectomy can be considered.
Back to the Case:
Case Resolution
In the case above, the patient’s ECG reveals several findings consistent with pericarditis, including diffuse ST elevation, PR depression, and Spodick’s sign. TTE demonstrated a moderate sized pericardial effusion without wall motion abnormalities or tamponade physiology. In this case, the patient’s history of SLE made a SLE-related pericarditis likely; this was further suggested by leukocytosis and temperatures >38°. Though the management of SLE-related pericarditis is beyond the scope of this guide, rheumatology was consulted and a prednisone taper was prescribed with symptomatic improvement within several days of initiation.
What is notable about this EKG?
It is critical to understand the differentiation of ST elevation myocardial infarction and acute pericarditis on ECG. Look for factors suggestive of STEMI first, including STE in III > II (for inferior STEMI) and reciprocal depressions. Then, look for factors suggestive of pericarditis, such as Spodick’s sign.
What do you think the patient is presenting with? What are the etiologies of this disease?
Most cases will be idiopathic in etiology, however it is important to ensure that secondary causes are considered, especially when patients have suggestive presenting features such as fever >38°C, leukocytosis in excess of 13,000, or a large pericardial effusion.
What is the management of this disease? Would you think of giving her steroids?
The management of acute pericarditis revolves around a short burst of NSAIDs and a longer course of colchicine, which has been associated with decreased recurrence in multiple studies. Glucocorticoids should be avoided as they increase risk of recurrence, and when used should be initiated at low doses.
What are the main complications of the disease?
Important to ensure that tamponade is not at play with pericarditis; though large effusions are uncommon, this is the most morbid acute complication. Constrictive pericarditis and recurrence pericarditis are other complications to keep in mind.
How’d we do?
The following individuals contributed to this topic: Mohsin Dohadwala, MD, Mary Rodriguez Ziccardi, MD
Chapter Resources
Mattu, Amal. “Amal Mattu's ECG Case of the Week – November 2, 2020.” ECG Weekly, 2 Nov. 2020, https://ecgweekly.com/2020/11/amal-mattus-ecg-case-of-the-week-november-2-2020/.
Witting, Michael D et al. “Evaluation of Spodick's Sign and Other Electrocardiographic Findings as Indicators of STEMI and Pericarditis.” The Journal of emergency medicine vol. 58,4 (2020): 562-569. doi:10.1016/j.jemermed.2020.01.017
LeWinter, Martin M. “Acute Pericarditis.” New England Journal of Medicine, vol. 371, no. 25, 2014, pp. 2410–2416., https://doi.org/10.1056/nejmcp1404070.
Chiabrando J, Bonaventura A, Vecchié A, et al. Management of Acute and Recurrent Pericarditis. J Am Coll Cardiol. 2020 Jan, 75 (1) 76–92.https://doi.org/10.1016/j.jacc.2019.11.021
Maisch, Bernhard et al. “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology.” European heart journal vol. 25,7 (2004): 587-610. doi:10.1016/j.ehj.2004.02.002
Loscalzo, Joseph, and Joseph Loscalzo. “Pericardial Disease.” Harrison’s Principles of Internal Medicine, Twenty-First Edition (Vol. 1 & Vol. 2), 21st ed., McGraw-Hill Education, 2022, pp. 2019–2025.