
Multisystem Involvement
Case Presentation:
A 62-year-old woman with a PMHx of HTN, HLD, CKD, and HFpEF was admitted to the CCU 3 days ago for ADHF. Over the past 2 months, she has become progressively more dyspneic on exertion along with increased LE edema. She endorses orthopnea, chest tightness and fatigue, but otherwise all ROS negative. Vitals: BP: 150- 170/80-90, HR: 90-110, O2 89% on RA, T: 98.6 F. Physical exam notable for increased work of breathing with diffuse bilateral crackles and holosystolic murmur loudest in the left lower sternal borders. JVD noted below the patient’s ear and 2+ pitting edema of lower legs. Labs significant for Cr of 2.4 (baseline 1.8-2.), BNP 5,987, high sensitivity trop 120→115. ABG showing pH 7.28, pO2 70, pCO2 60, HCO3 28 with negative respiratory viral panel. CXR showing cardiomegaly with increased pulmonary venous congestion and interstitial edema, while CTA negative for PE..
Ask Yourself:
Questions:
1. How is pulmonary hypertension (PH) defined and classified? What class of PH does this patient fall into?
2. What findings on this patient’s non-invasive workup are suggestive of PH? Can any of these modalities effectively rule in or out PH?
3. When should a right heart catheterization (RHC) be pursued for the evaluation of PH? Why was a RHC performed on this patient?
4. How does a diagnosis of PH affect the management of patients with heart failure? How should this patient be managed?
TTE was done and showed similar left ventricular hypertrophy with mild diastolic dysfunction and EF of 50-55% (similar to prior). New right ventricular (RV) mild-moderate concentric hypertrophy with normal systolic function and mildly dilated right atrium (RA). New tricuspid valve regurgitation with a peak velocity of 3.2 m/s with estimated pulmonary arterial systolic pressure (PASP) of 47 mmHg. There is also notable systolic flattening of the interventricular septum. Inferior vena cava (IVC) 2.2 cm with <50% collapse on inspiration.
Based on the above ECHO findings, a decision was made to pursue a right heart catheterization:
Right Heart Catheterization (RHC):
Right Arterial Pressure (RAP): 8 mm Hg (ref: 0-7 mm Hg)
Pulmonary Arterial Systolic Pressure (PASP): 47 /16 mm Hg (35) (ref: 17- 32 mm Hg)
Mean Pulmonary Arterial Pressure (mPAP): 35mm Hg (ref: 9-19 mm Hg)
Pulmonary Capillary Wedge Pressure (PCWP): 16 mm Hg (ref: 4-12 mm Hg)
Pulmonary Vascular resistance (PVR): 3.58 wood units (ref: < 2 wood units)
Cardiac Output (CO): 5.3 L/min (ref: 3-5 L/min)
Cardiac index (CI): 2.8 (ref: 2.8- 4.2)
Background:
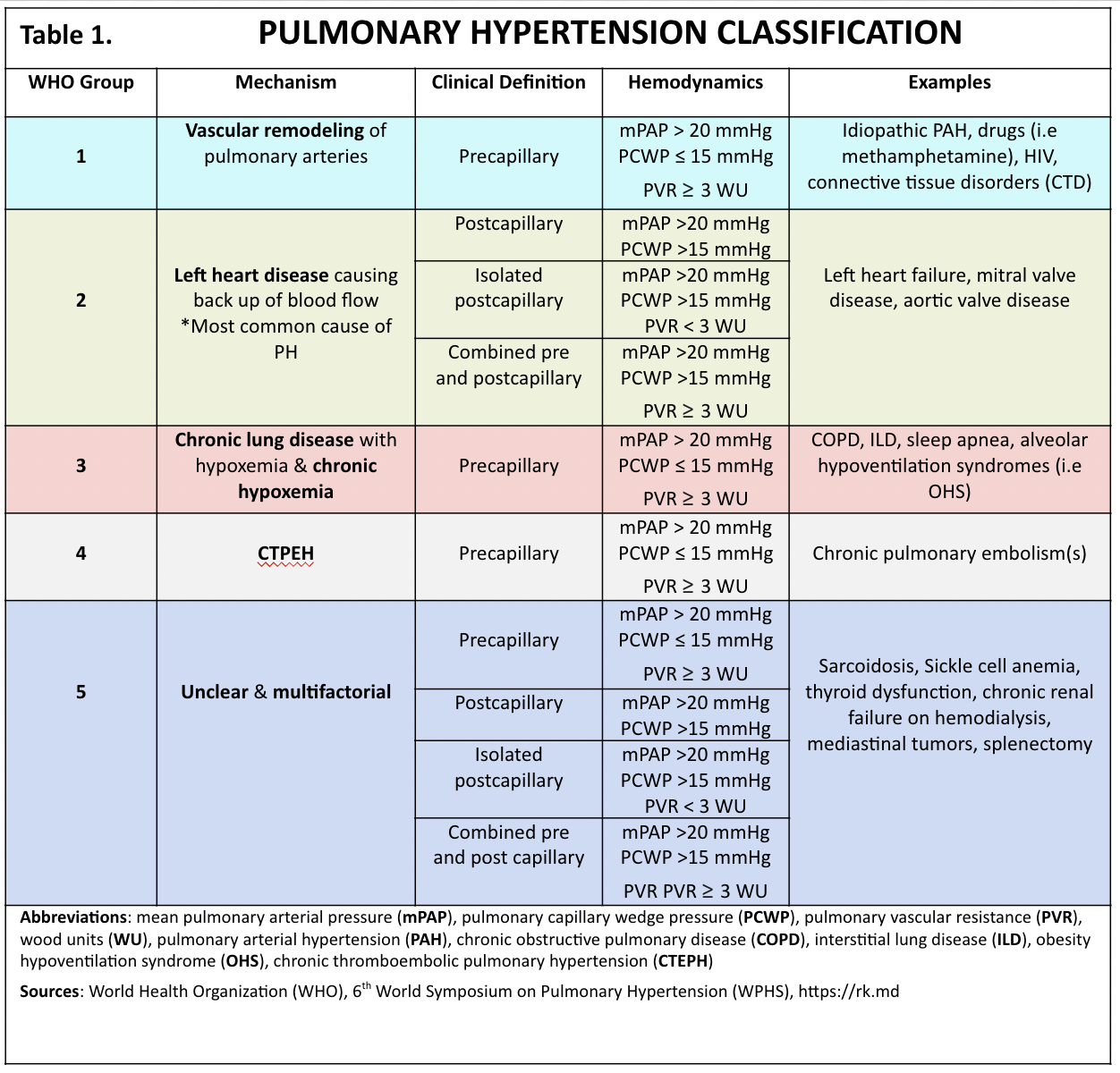
Pulmonary Hypertension (PH) is defined by elevated blood pressure within the pulmonary vasculature. Specifically, the Mean Pulmonary Arterial Pressure (mPAP) > 20 mm Hg at rest
Defining and Classifying PH
→ The World Health Organization (WHO) classifies PH into 5 groups based on the underlying etiology or mechanism (Table 1).
→ PH is further defined by the location of the disease process within the pulmonary vasculature causing elevated PA pressures and the relative hemodynamics involved.
-Pre-capillary: due to a primary elevation in the pulmonary arterial system alone. Defined by a pulmonary vascular resistance (PVR) ≥ 3 wood units (WU). PVR = (mPAP – PCWP)/ CO (unit = dynes/sec/cm5)
- Post-capillary: due to elevated pressures in the pulmonary venous system. Defined by a PCWP (or pulmonary arterial occlusion pressure (PAOP)) > 15 mm HG. PCWP/PAOP provides an estimate of left atrial pressure due to the high compliance of pulmonary circulation. Includes patients with PH due to left heart disease (PH-LHD)
- Combined: due to the passive transmission of increased left-sided filling pressures with superimposed pulmonary vascular disease (Cpc-PH). Elevation in mPAP is "disproportionate" to that generated by the transmission of increased left-sided filling pressures alone. PCWP >15mm HG and a Transpulmonary Gradient (mPAP- PCWP) >12 mmHG or diastolic pressure gradient (diastolic PAP- PCWP) > 7mmHg. Often associated with a PVR ≥ 3 WU
Signs and Symptoms
Clinical Symptoms and Physical Exam Findings of PH
→ Initial Presentation:
- Exertional dyspnea, lethargy, fatigue
- Loud P2 (pulmonic component of S2 during inspiration)
→ Progression to RV failure
- Exertional chest pain and syncope
- Weight gain from edema
- Anorexia and/or abdominal pain from hepatic congestion
- JVD, wide splitting of second heart sound, holosystolic murmur of tricuspid regurgitation
- Hepatomegaly, peripheral edema, ascites, pleural effusions


CXR (see figure 3): Enlarged central pulmonary arteries (arrowheads, A), peripheral hypovascularity (large arrows, A); RA dilation (prominent right heart border (short arrow, A)); RV dilation (diminished retrosternal space (block arrow, B)).
CT/CTA Chest: CT may demonstrate similar findings to CXR but in greater detail. Main PA/ascending aorta diameter ratio ≥ 1 suggests PH. PE on CTA may indicate CTEPH.

Potential EKG & Image Findings in Patient with PH
EKG: May show signs of right ventricular hypertrophy (RVH) or right heart strain such as right-axis deviation and incomplete or complete right bundle branch block (RBBB) (Figure 2)
Diagnosis and Evaluation of Suspected Pulmonary Hypertension
→ Initial test of choice is Transthoracic Echocardiography (TTE). Specific TTE findings suggest the probability of PH and determine the need for further testing (see Table 2 & 3)
Peak tricuspid regurgitation velocity (TRV) > 2.8 m/s indicates possible PH
TRV > 3.4 m/s indicates a high probability of PH
If TRV ≤ 3.4 m/s, probability of PH is determined by the presence of other “PH signs” on TTE
→ Initial evaluation focuses on determining the presence and degree of left heart disease (LHD)

If there is sufficient LHD to explain the increase in mPAP then additional invasive testing is not needed unless otherwise indicated (see below section on indications for RHC)
Quantifying what constitutes “sufficient LHD” is challenging:
Typically, a dilated LA is indicative of chronically elevated LA pressure and supports PH due to LHD.
The 6th WPHS proposed an evaluation combining TTE and clinical findings with other risk factors to predict the probably of sufficient LHD (figure 3, see below)
High probability- typically do not need a RHC
Intermediate probability- typically need a RHC
Low probability- need additional testing tailored to potential causes of PH

If there is no LHD or insufficient LHD to explain the degree of elevation in mPAP then additional testing (noninvasive or RHC) is indicated to identify the cause of PH
Selection and sequence of additional testing varies based on clinical suspicion for the etiology of PH, but testing for the most common causes is usually pursued first:
CLD and hypoxemia (group 3)
Pulmonary function test (PFT), High Resolution CT chest (HRCT), 6-minute walk test, sleep study
Low DLCO on PFTs is sensitive but not specific for PH
-If severity of pulmonary dysfunction can explain degree of PH on TTE then RHC may not be necessary
CTEPH (group 4)
V/Q scan (usual first choice), CT angiography (CTA)
Can be clinically diagnosed without RHC if PH is evident on TTE and V/Q scan has clear evidence of thromboembolic disease
In the absence of PA obstruction or CLD and/or chronic hypoxemia other etiologies should be assessed
PAH (group 1)
HIV testing, liver function (portal hypertension), medications/toxins, congenital heart disease, connective tissue disease (CTD)
RHC indicated
Rare multifactorial causes (Group 5)
Sarcoidosis, sickle cell, mediastinal tumors
Groups of Pulmonary Hypertension:

PAH (Group 1)
Calcium Channel Blocker (CCB) therapy
Indicated in PAH with a positive vasoreactive response to short-acting vasodilators (ie. nitric oxide, adenosine) during a RHC. A positive response will increase mean pulmonary artery pressure by > 10 mmHg with total value < 40 mmHg
AVT testing is indicated in only 10-20% of PAH subsets: Idiopathic, heritable, drug/toxin-induced
All other etiologies (ex. HIV-induced, CTD) are unlikely to be vasoreactive
PAH-directed therapy
Medications that directly treat PH by lowering PVR and PAP
Prostacyclin agonists/prostanoids (exp. Treprostinil, Epoprostenol)
Endothelin antagonists (exp. Ambrisentan, Macitentan)
Phosphodiesterase 5 (PDE5) inhibitors (exp. Sildenafil, tadalafil)
Soluble guanylate cyclase stimulator (exp. Riociguat)
Indications
PAH without vasoreactivity or with vasoreactivity but a failed response to CCB
Decision to start therapy and specific regimens depends on patient functionality
Diuretics are beneficial in volume overload but can theoretically precipitate an acute PH crisis if volume depletion leads to hypotension
LHD (Group 2)
Optimize management of LHD
Titrate to target doses of GDMT
Decongest with diuretics as needed
Treatment of ischemic and valvular heart disease with surgical or transcatheter interventions
Device therapies including cardiac resynchronization
In patients with PH-LHD
PAH-directed therapy is not recommended for routine use and can cause acute pulmonary edema by increasing blood flow into a noncompliant LA and LV
In patients with Cpc-PH
Treatment involves unloading the left heart
Control blood pressure, diuretics as needed, etc.
Decreasing left sided pressures will decrease afterload on the RV which can allow pulmonary vasculature to remodel over time
Low doses of PDE-5 therapy may be used as a last option if RV dysfunction is present and symptoms of PH persist despite near normal PCWP
CLD and/or hypoxemia (Group 3)
Treat underlying disease: Inhaler therapy, CPAP, lung transplant in severe cases
For most patients in group 3, PAH-directed therapy is not recommended
Can cause hypoxia and decrease quality of life in COPD
ILD patients with pre-capillary PH and PVR > 3WU may benefit from inhaled treprostinil
CTEPH (Group 4)
Surgical treatment with Pulmonary thromboendarterectomy (PTE) is potentially curative
PAH-directed therapy may be indicated in inoperable CTEPH or persistent CTEPH following PTE (riociguat is 1st line)
Rare multifactorial causes (Group 5): Treat underlying disorder
PH Complications
Cor pulmonale - RV enlargement and/or impaired function
Right heart failure (RHF)/RV dysfunction is one of the strongest predictors for adverse outcomes in HFrEF, HFpEF, and non-HF-related PH
Acute PH crisis – Acute increase in pulmonary vascular resistance leading to acute RHF, decreased cardiac output (CO), and shock.
Triggers: hypovolemia, acute lung disease, increased cardiac demand, interruptions in continuous prostanoid infusions, arrythmias
Management: consult PH specialist, promptly resume the temporarily discontinued prostanoid, maintain euvolemia, administer inotropic and/or vasopressor support to augment CO if necessary
Take caution with inotrope induced hypovolemia (levophed is typically started before dobutamine to avoid hypotension, then titrated down as tolerated)
Arrhythmias – increased risk in PAH
Most common: SVT, A-fib, A-flutter
Can also have bradycardia due to RV dilation
Early management (medication, cardioversion, ablation etc.) is important to reduce risk of precipitating an acute PH crisis
PH-LHD is associated with increased morbidity and mortality compared to LHD without PH.
Treatment for PH depends on the etiology and functional severity of the disease . All groups of PH can benefit from conventional and supportive therapies such as exercise, smoking cessation, vaccination, supplemental O2 if hypoxic, and diuretics if volume overloaded.
Back to the Case:
1. Which class of PH does this patient fall under?
This 62-year-old patient with HTN and HLD presenting in ADHF with TTE findings of LVH and diastolic dysfunction has an intermediate risk of PH secondary to LHD. Her PCWP of 16 confirms a post-capillary etiology.
However, her persistent hypoxemia despite diuresis and clear lung fields may suggest a secondary disease process. Her PVR of 3.57 WU also indicates a pre-capillary component to her PH.
Answer: WSPH group 2, Combined pre- and post-capillary (Cpc-PH)
Additional investigation should be pursued to determine the etiology of the pre-capillary component to her PH
2. What findings on this patient’s non-invasive work up are suggestive of PH? Can any of these modalities effectively rule in or out the diagnosis of PH?
Physical Exam:
A loud S2 heard on auscultation could represent an intensified P2 which is concerning for PH.
A holosystolic murmur heard loudest in the left lower sternal border is characteristic for tricuspid regurgitation which can be caused by elevated pulmonary pressures.
EKG:
The peaked R waves in V5-V6 and T-wave inversions (TWI) in the lateral leads of the old and current EKG suggest LVH; however, there is now an rSR’ pattern (M-shape) in V1 (C1) in the setting of TWI in V1-V3 suggesting a new RBBB.
Patients with PH may or may not develop signs of RV disease (R-axis deviation, RVH, RBBB, etc.) on EKG. PH cannot be ruled in or out solely based on EKG results
TTE:
The new tricuspid valve regurgitation (TVR) with a peak velocity of 3.2 m/s in the setting of other “PH signs”, including an IVC of 2.2 cm with <50% inspiratory collapse and systolic flattening of the interventricular septum gives her a high probability of PH.
3. When should a RHC be pursued for the evaluation of PH? What is the likely reason a RHC was performed on this patient?
A RHC should be ordered when the presence, etiology or severity of PH is unclear despite initial noninvasive testing.
Based on this patient’s age, metabolic factors, EKG findings of LVH, and TTE with mild diastolic dysfunction and a non-dilated LA she has an intermediate probability that her PH is solely due to LHD. Since her TTE suggests moderate PH based on the PASP of 47 mm HG and she is still experiencing dyspnea and hypoxia despite optimization of her LHD a RHC is indicated.
4. How does a diagnosis of PH affect the management of patients with known left heart failure? How should this patient be managed?
Treatment of PH in patients with LHD depends on the etiology of the PH. In PH-LHD management entails optimization of LHD. In Cpc-PH, management might differ depending on the etiology of the superimposed pulmonary vascular disease but typically entails treating the underlying pathology.
This patients RHC diagnosed Cpc-PH, which more often than not is still related to LHD, but could indicate a second disease process that should be evaluated.
She should be referred for additional testing, such as PFTs and/or HRCT
A more complete history, including family history, and medication review should be obtained to assess for potential genetic, autoimmune (i.e sarcoidosis), or infectious (i.e HIV) etiologies and related work up.
A referral to pulmonology or a PH specialist is indicated
Further Learning:
Key Learning Points:
Suspect PH in patients with progressive or unexplained dyspnea and/or fatigue on exertion and/or signs of right heart dysfunction (i.e. peripheral edema, ascites, signs of RVH on EKG or CXR).
PH is classified by its underlying etiology (WSPH group) and whether that etiology causes elevated PAP directly by affecting the pulmonary arteries (pre-capillary), indirectly by increasing pulmonary venous pressure (post-capillary), or mixed pre- and post-capillary disease.
Left Heart Disease (LHD) is the most common cause of PH, but many patients have other risk factors for superimposed pulmonary vascular disease (i.e. COPD, thromboembolic disease, HIV) to keep in mind.
A TTE is the initial test of choice for suspected PH. It predicts the probability of PH using peak TRV along with the presence of other “PH signs” (ex. RA/RV enlargement, dilated IVC), provides hemodynamic values that when combined with other clinical factors can help determine if LHD is sufficient to explain the degree of PH (figure 2), and directs need for additional testing
If the severity of LHD cannot explain the degree of PH then additional testing should be pursued to determine the etiology of PH. Consider other common causes:
If CLD is suspected, check for PFTs with signs of obstructive or restrictive disease with a reduced DLCO. HRCT can also be used to detect findings of ILD.
If the patient has a history of thromboembolism, especially PE, assess for CTEPH with a V/Q scan and/or CTA chest.
RHC is the gold standard diagnostic exam for PH, but it is not always necessary. Order when the presence, etiology or severity of PH is unclear despite initial noninvasive testing. RHC can provide mPAP to confirm diagnosis of PH (mPAP > 20 mm hg), as well as PCWP and PVR to further confirm or evaluate for a pre- or post-capillary etiology of PH (figure 1)
Treatment of PH depends on the etiology and functional severity of the PH, and typically involves optimization and treatment of the underlying etiology. PAH-directed therapy (ex. sildenafil, ambrisentan) is usually only indicated in Group 1 PH (with some exceptions) and should be managed by a PH specialist.
Treating PH-LHD involves optimization of LHD with titration of GDMT to goal, achieving euvolemia, and timely correction of any arrhythmias or valvular dysfunction. In PH-LHD treatment with PAH-direct therapy is not recommended and can cause acute pulmonary edema if LHD is not optimized
Major complications of PH include chronic RHF (cor pulmonale), acute RHF (PH crisis) and increased chance of arrhythmias
Abrupt cessation of PAH-directed therapy can induce a PH crisis in which case the therapy should be restarted immediately
Over diuresis and hypovolemia can theoretically induce a PH crisis in patients with pre-capillary PH; however, usually patients with PH and cor pulmonale are hypervolemic and require diuresis.
Resident Responsibilities:
Be able to recognize the symptoms of PH, especially those associated with acute RHF (PH crisis) as this is an emergency that should involve a PH specialist or may require transport to a PH care center.
In a patient with a PH diagnosis, know the etiology as it may affect management.
If PH is demonstrated on TTE, be sure to have a conversation regarding the likelihood it is solely induced by LHD or if further testing with a RHC is indicated.
Ensure patients with LHD-PH are optimized by titrating GDMT to goal, diuresing to euvolemia if overloaded, and controlling arrhythmias.
Attending Pearls (per Dr. Dustin Fraidenberg):
Pulmonary hypertension is a severe disease in all of its classifications/groups and needs to be treated as such, early recognition and timely diagnostic testing can make a huge difference on patient care.
Pulmonary hypertension specific treatments should be continued at all times unless there is a clear indication to hold them, any questions or concerns regarding treatment should be directed to a PH specialist.
If in doubt, diurese, right heart failure, much like left heart failure, is a disease of pressure and volume overload. Over-diuresis is very rare and most patients with chronic PH will also have chronic cor pulmonale and chronic hypervolemia. Assessments such as signs of hypervolemia (JVD, LE edema), BNP levels, bedside ultrasound IVC measurements and other markers of intravascular volume can help determine how best to manage volume.
How’d we do?
The following individuals contributed to this topic: Kristin Auge-Bonersky, MD, Dustin Fraidenberg
Chapter Resources
Rubin LJ, Hopkins W. Clinical features and diagnosis of pulmonary hypertension of unclear etiology in adults. Post TW, ed. UpToDate. Waltham, MA: UpToDate Inc.
Francis J. Right bundle branch block and left ventricular hypertrophy – All About Cardiovascular System and Disorders. Accessed March 28, 2023. https://johnsonfrancis.org/professional/rbbb-and-lvh/
Deng, J. Clinical application of pulmonary vascular resistance in patients with pulmonary arterial hypertension. J Cardiothorac Surg 16, 311 (2021). https://doi.org/10.1186/s13019-021-01696-4
Ibe T, Wada H, Sakakura K, et al. Combined pre- and post-capillary pulmonary hypertension: The clinical implications for patients with heart failure. PLoS One. 2021;16(3):e0247987. Published 2021 Mar 2. doi:10.1371/journal.pone.0247987
1. The 6th World Symposium on ph: Hemodynamic definitions and updated clinical classification of ph (part 1). American College of Cardiology. Accessed May 31, 2023. https://www.acc.org/latest-in-cardiology/articles/2019/10/30/08/08/the-6th-world-symposium-on-ph-part-1.
Fraidenburg, D.R., Yuan, J.XJ., Gaine, S.P. (2015). Diagnosis and Treatment of Pulmonary Arterial Hypertension. In: Lanzer, P. (eds) PanVascular Medicine. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-37078-6_155